🗓️ Unit 12
Psychological Disorders
PSYC 181 – Intro to Psych
August 12, 2024
What you will learn
![]()
Learning Objectives
Describe the historical and modern approaches to mental health services and treatment
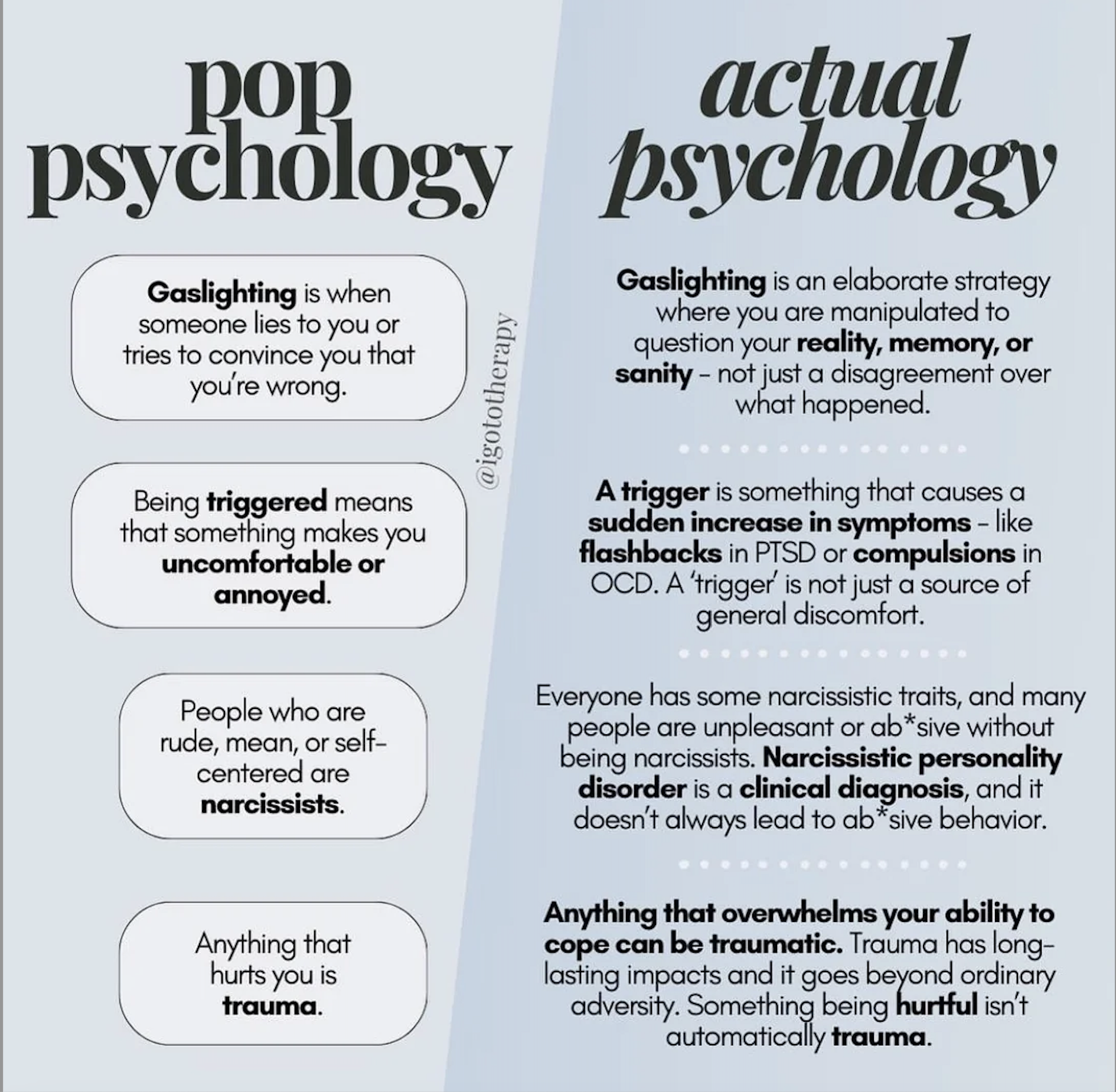
Understand the problems inherent in defining the concept of psychological disorder
Describe what is meant by harmful dysfunction
Identify the formal criteria that thoughts, feelings, and behaviors must meet to be considered abnormal and, thus, symptomatic of a psychological disorder
Treatment in the past
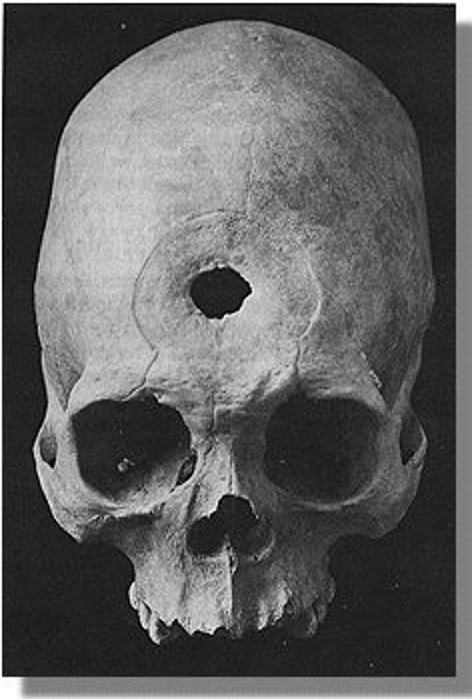
18th Century
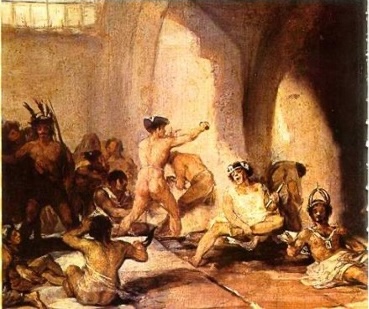
Phillippe Pinel (Late 1700’s)

Dorothea Dix (19th Century)

- Social reformer and advocate for indigent insane
- Identified poor state of care
- Instrumental in first American mental asylum
American Asylums (19th Century)

- Usually filthy
- Limited treatment
- Individuals often institutionalized for decades
20th Century


Mental Health Treatment Today


Psychotherapy psychological treatment that employs various methods to help someone overcome personal problems, or to attain personal growth

Play Therapy

Exposure Therapy
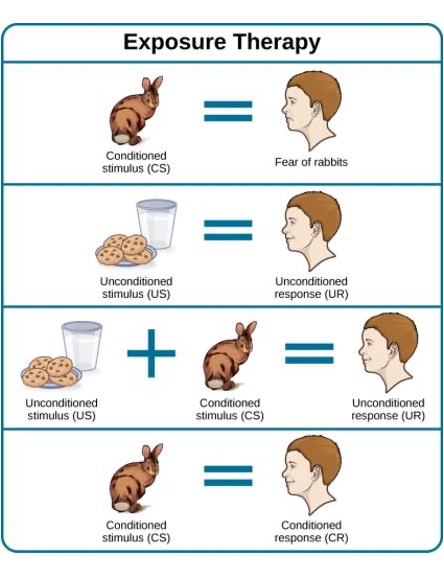
Systematic Desensitization
- Type of exposure therapy wherein a calm and pleasant state is gradually associated with increasing levels of anxiety-inducing stimuli

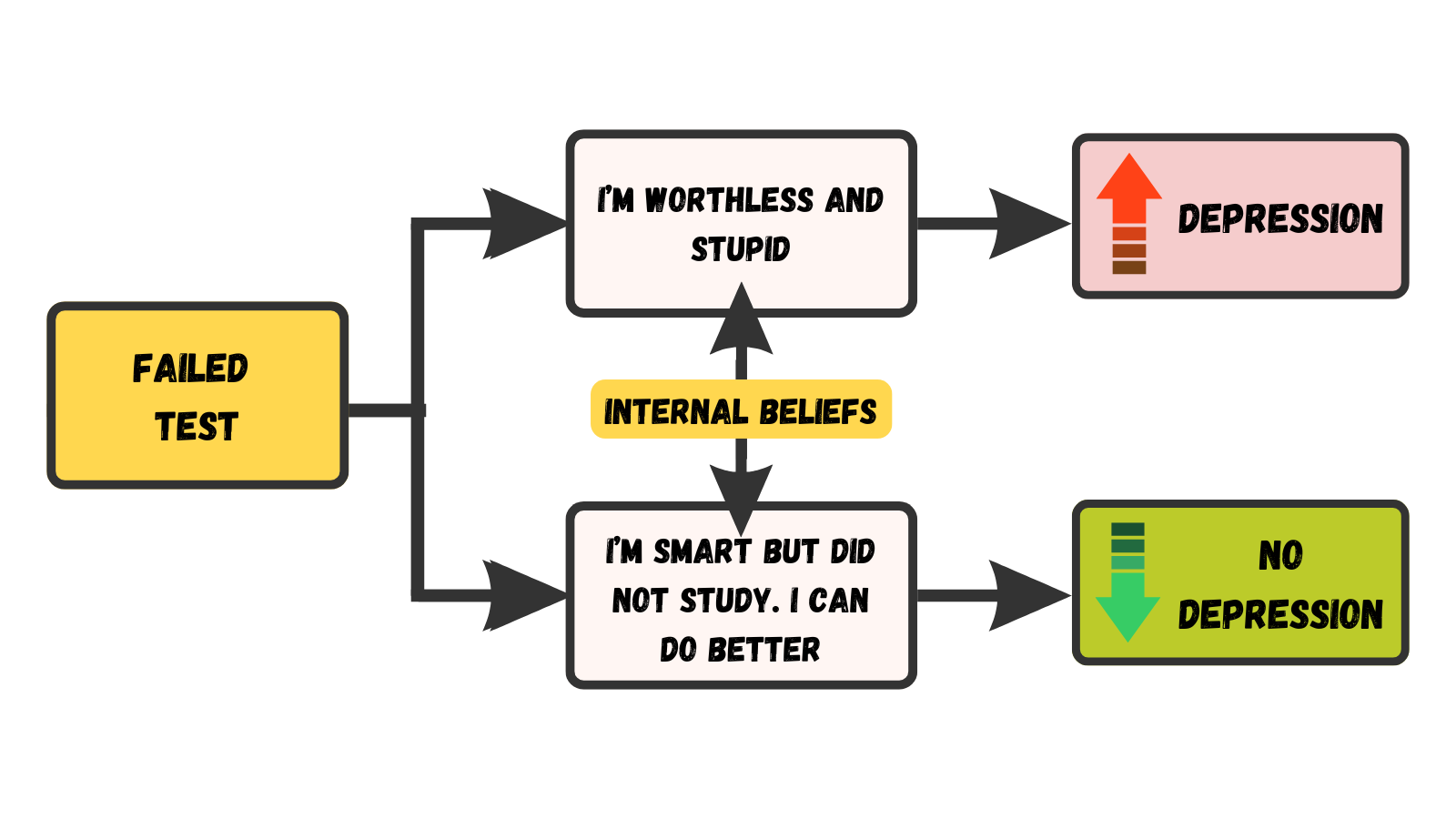
Cognitive-behavioral Therapy
THE DIAGNOSTIC & STATISTICAL MANUAL OF MENTAL DISORDERS (DSM)
Diagnosis appropriately identifying and labeling a set of defined symptoms
- Requires classification systems that organize psychological disorders systematically
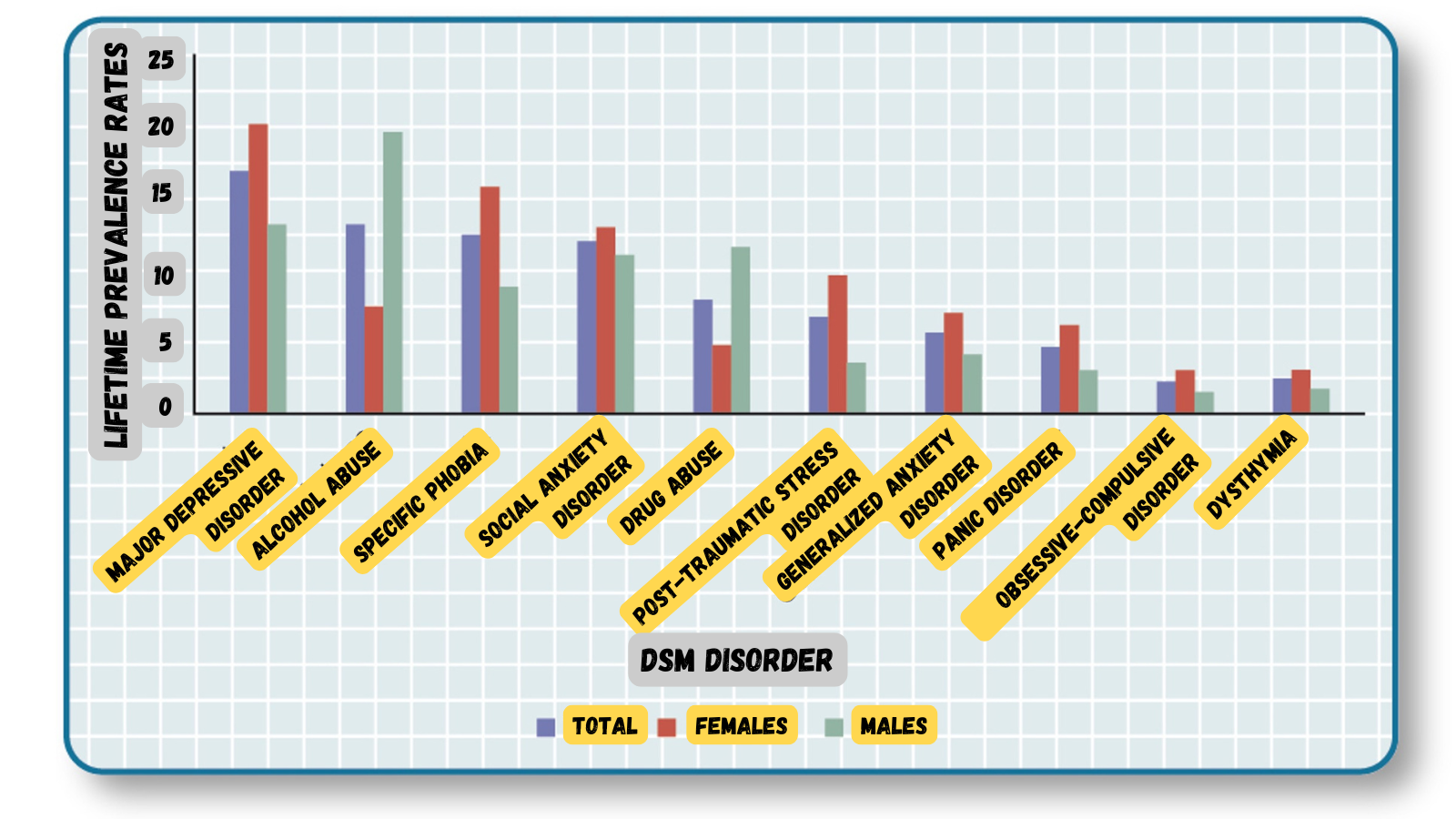
PREVALENCE RATES (DSM-IV)
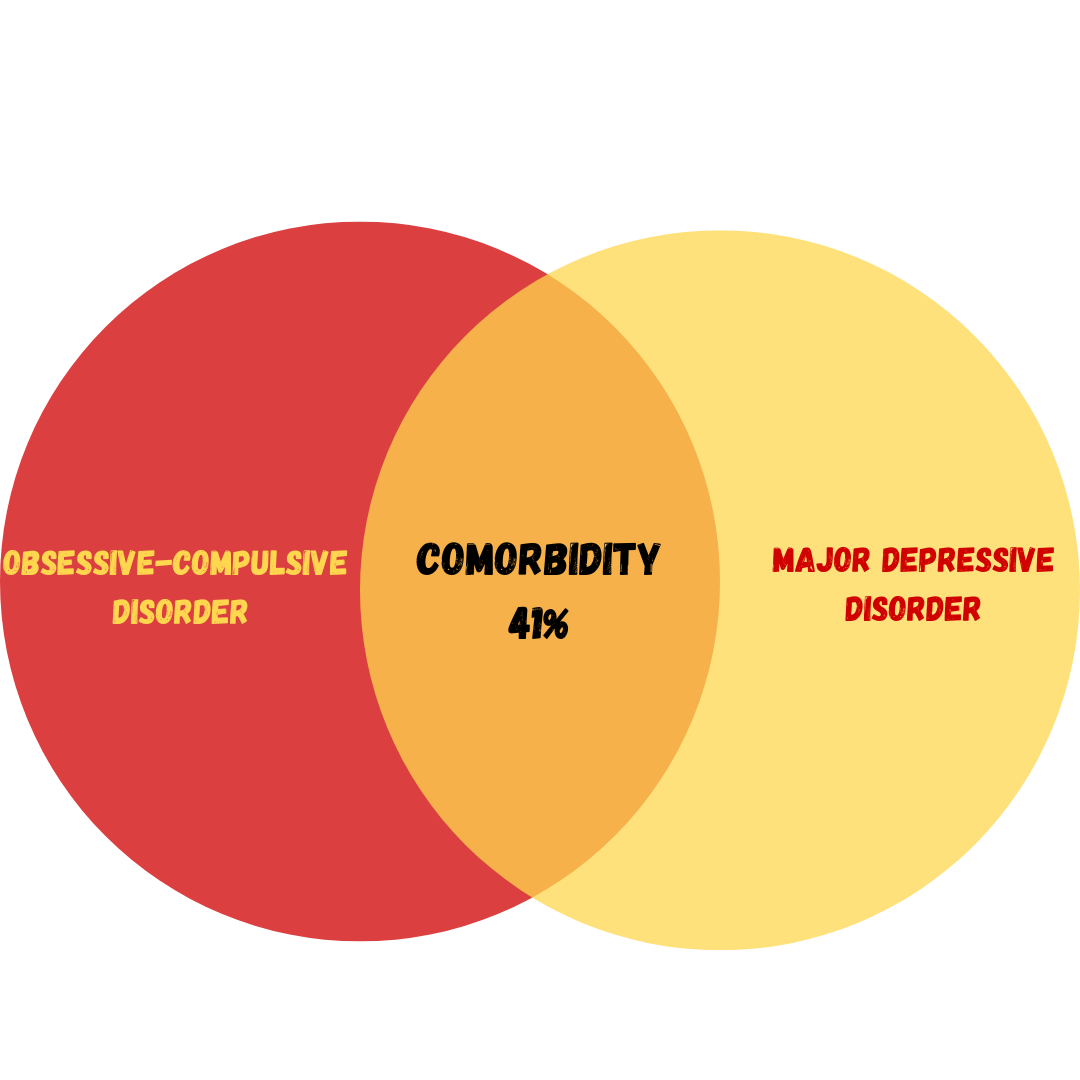
COMORBIDITY (DSM)
SUPERNATURAL PERSPECTIVES

Disorders attributed to a force beyond scientific understanding
- Practitioners of black magic (sorcery)
- Possessed by spirits
- Witchcraft
DANCING MANIA


BIOLOGICAL PERSPECTIVES
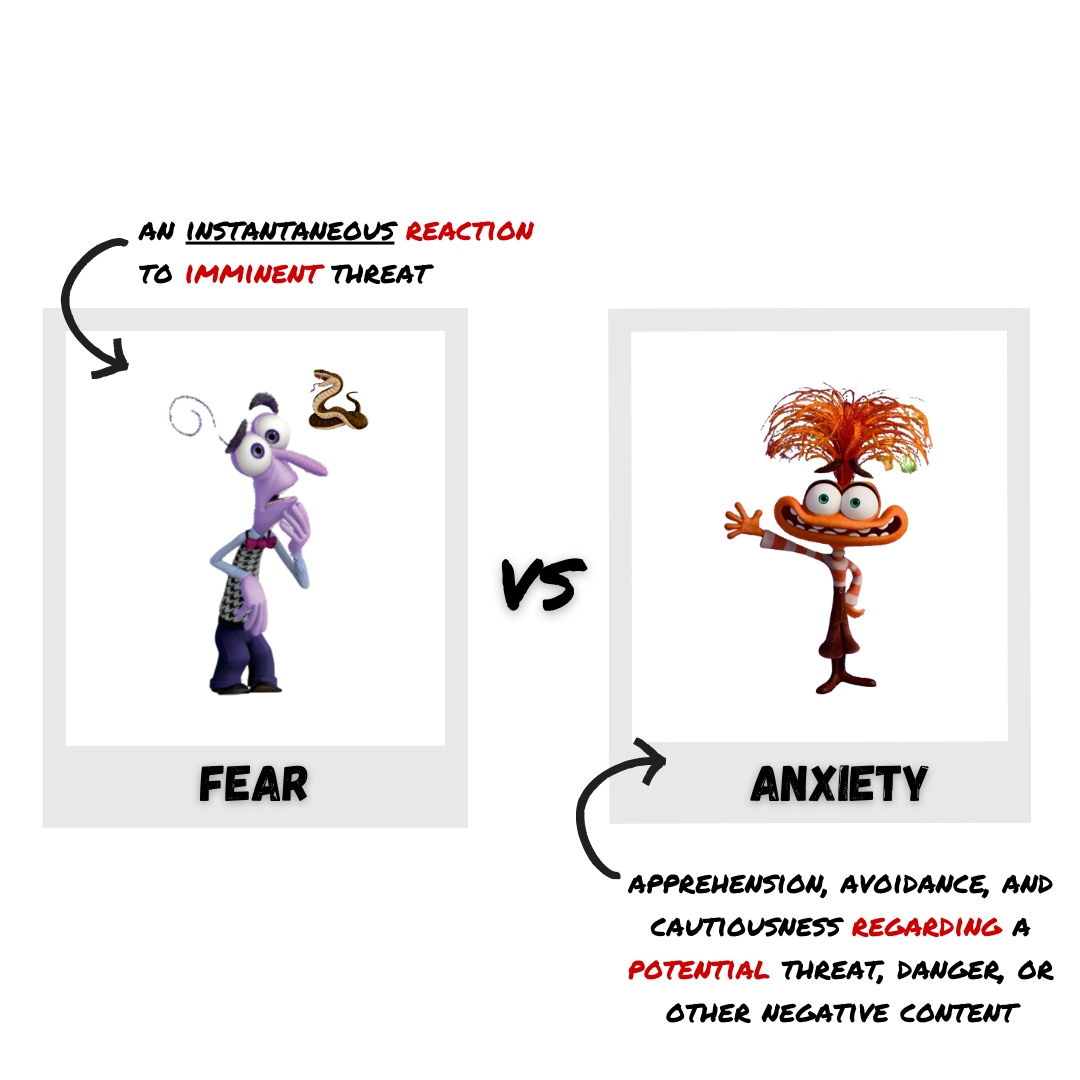
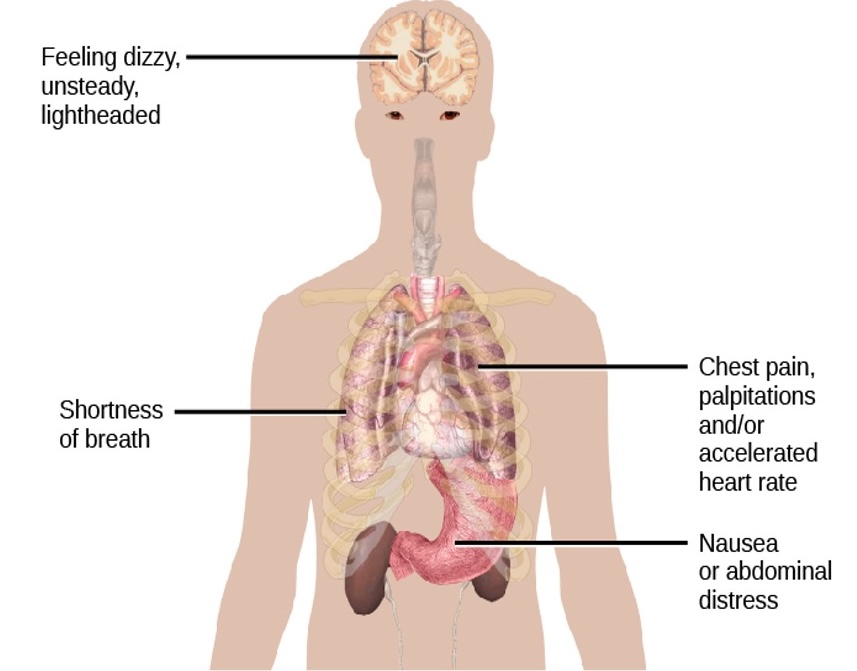
Anxiety
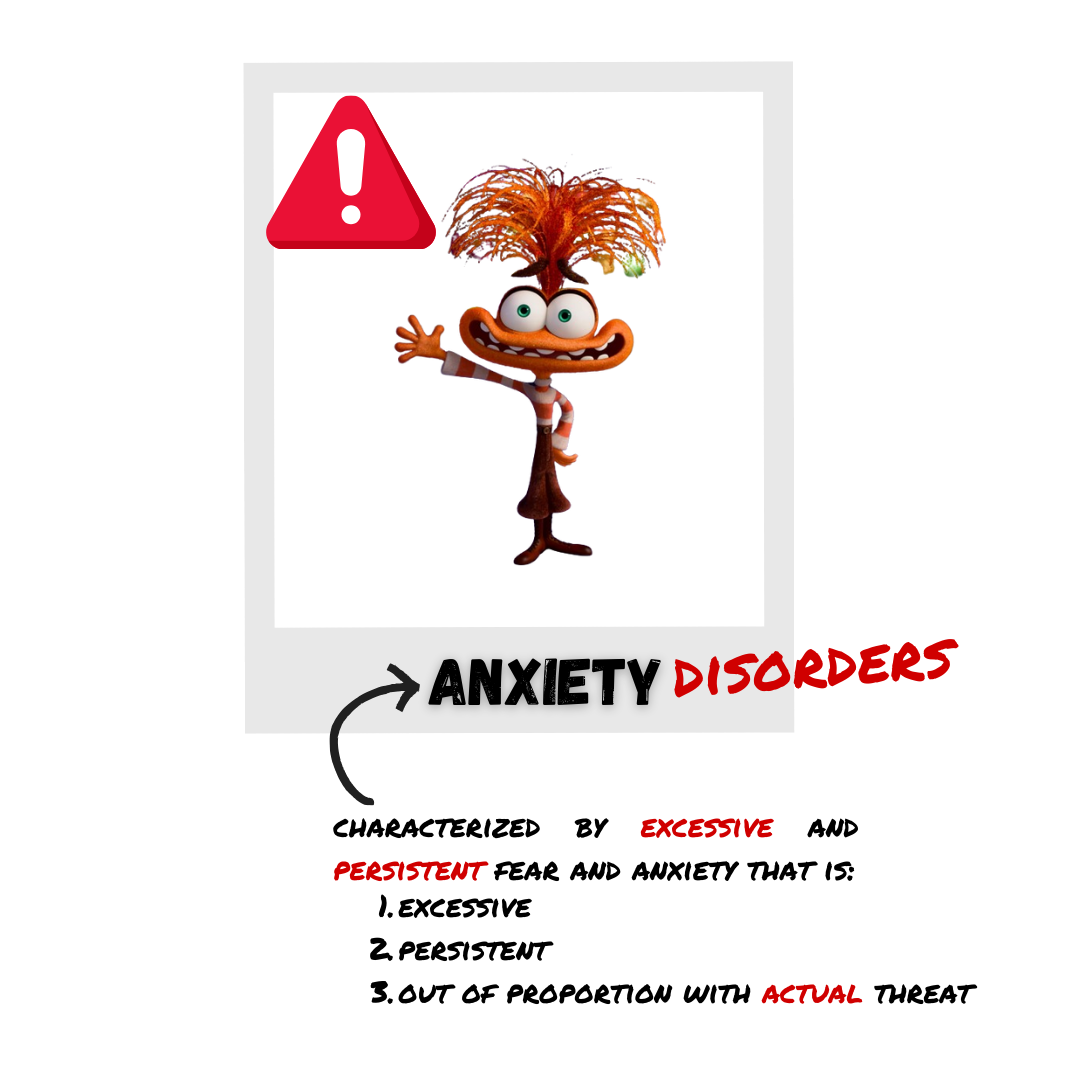
Anxiety Disorders
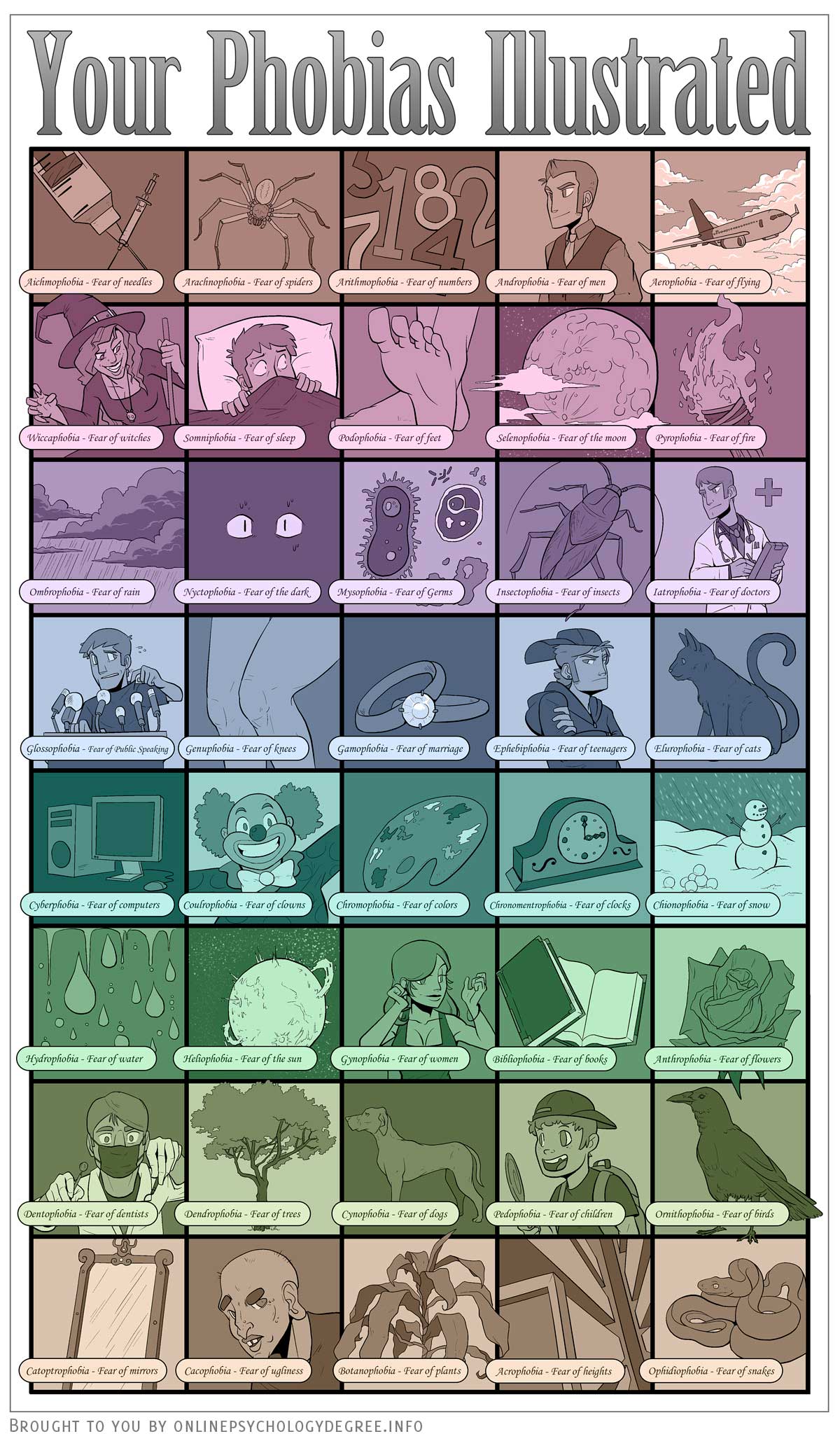
Common Phobias
PANIC DISORDER
Prevalence
- ~ 12% of U.S. population
Comorbidity
- anxiety or major depressive disorders
OCD Circuit
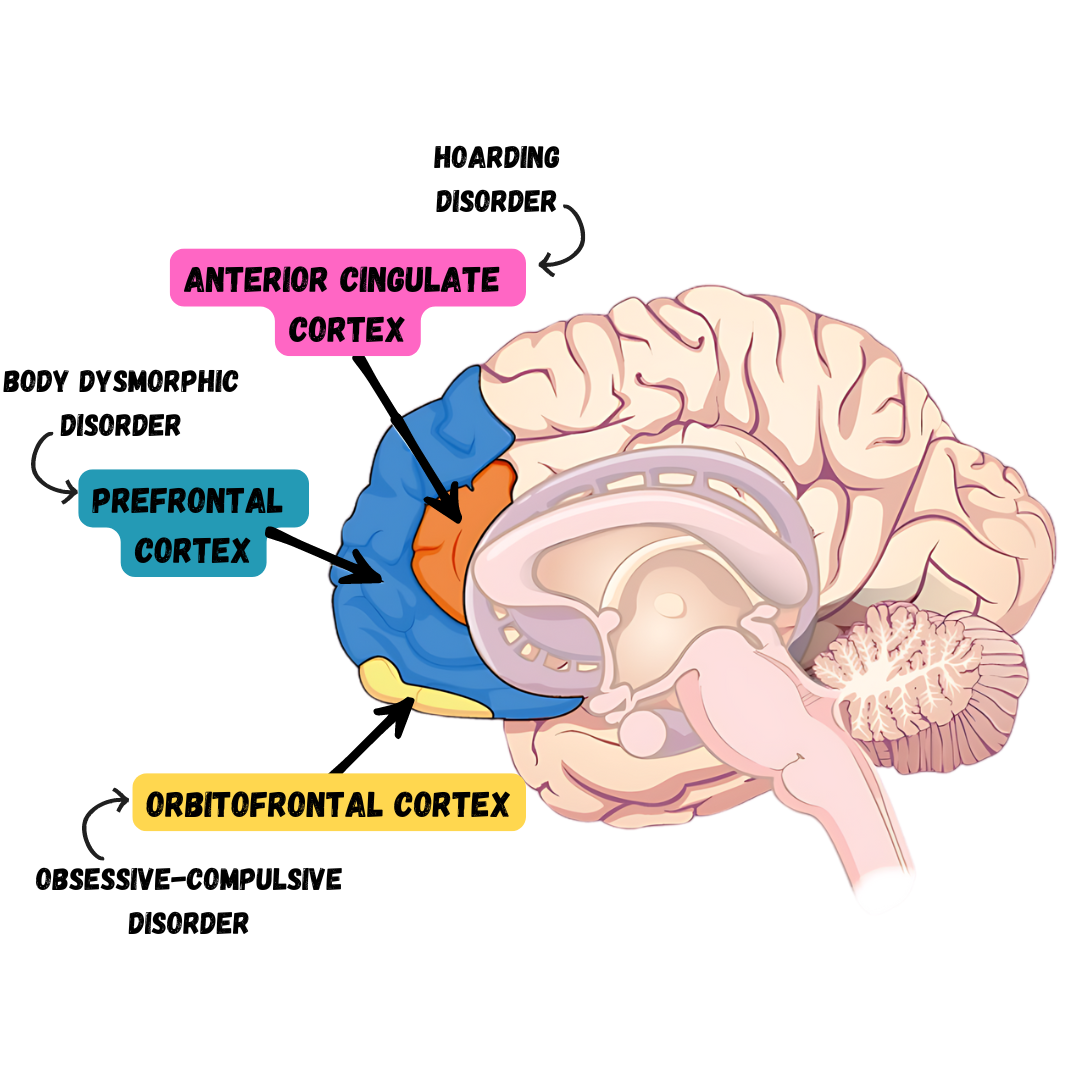
Orbitofrontal cortex
- involved in learning and decision making
- Becomes hyperactive in people with OCD when provoked with tasks such as looking at photos of a toilet or a pictures hanging crookedly on a wall
HOARDING DISORDER

BIOLOGICAL BASIS OF MOOD DISORDERS
Hormones
Elevated levels of cortisol (stress hormone) are found in depression
Cortisol activates the amygdala and deactivates the prefrontal cortex (disturbances connected to depression)
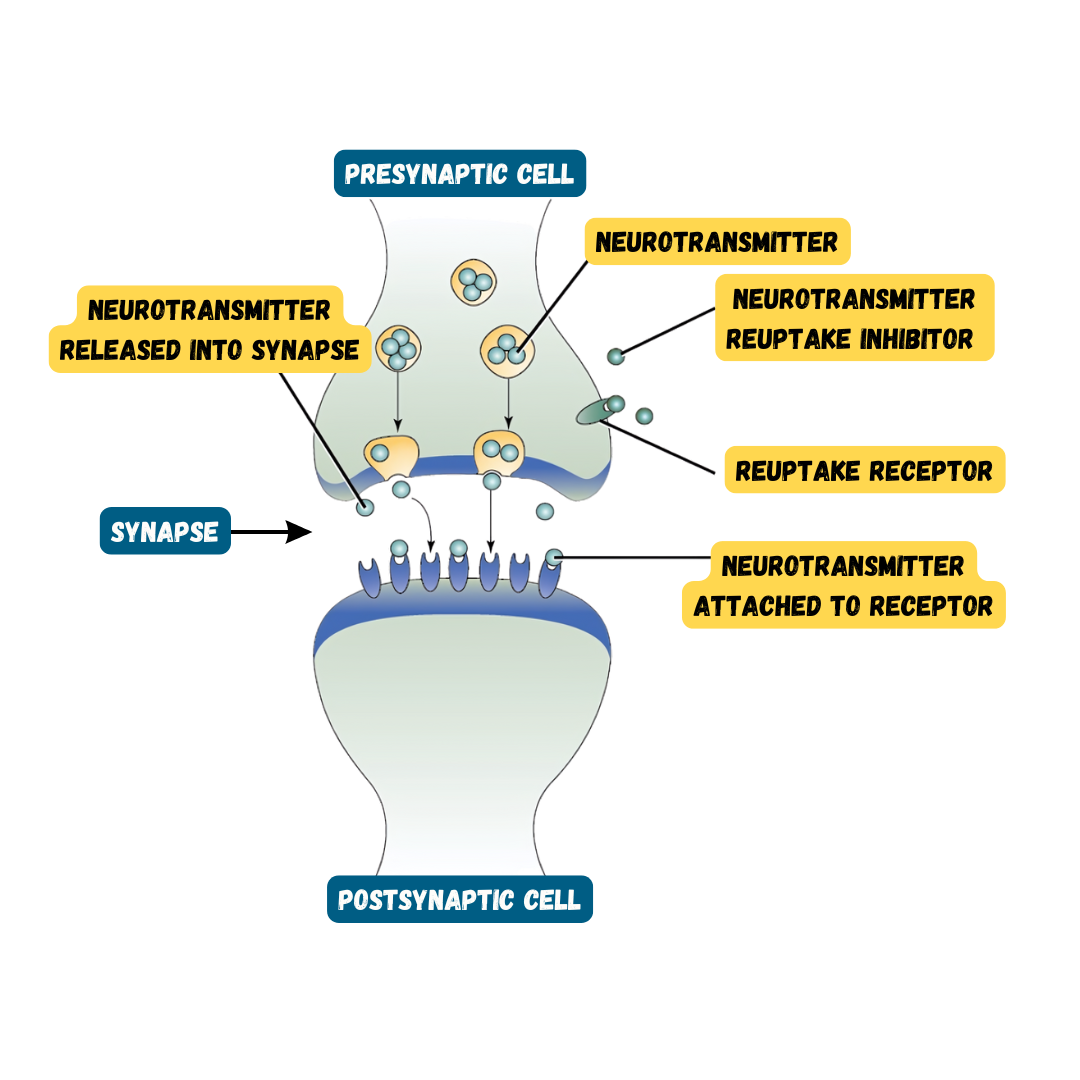
Neurotransmitters
Mood disorders often involve imbalances in neurotransmitters
Particularly serotonin and norepinephrine
Many medications work by altering balance
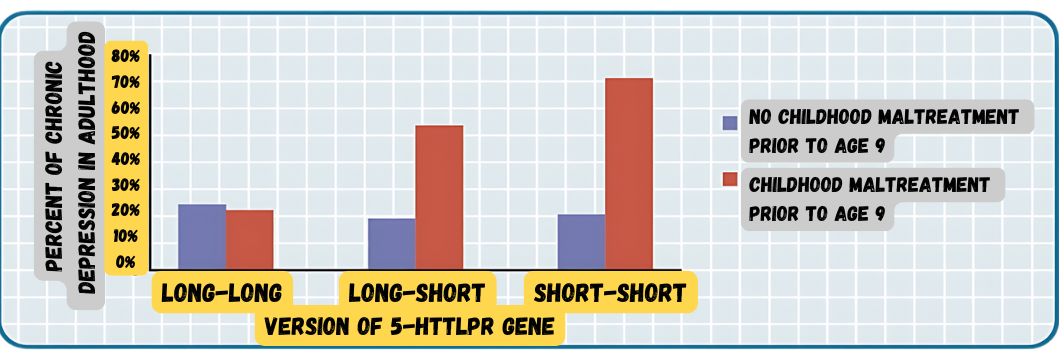
DIATHESIS-STRESS MODEL & MAJOR DEPRESSIVE DISORDERS
- Stressful life events often precede the onset of depressive episodes
ANTISOCIAL PERSONALITY DISORDER
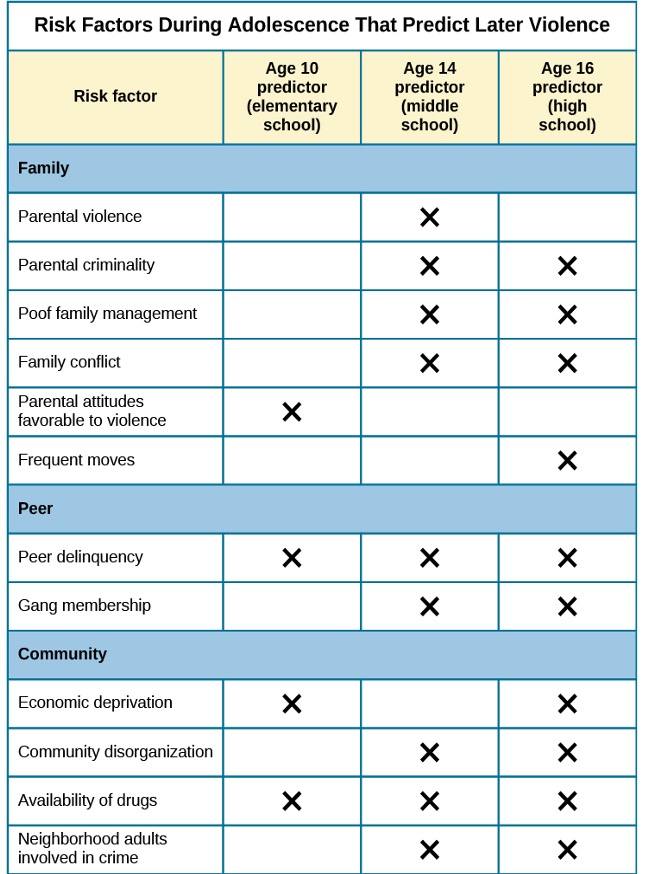
Symptoms
Repeatedly performing illegal acts=
Lying to or conning others
Impulsivity and recklessness
Irritability and aggressiveness
Failure to act in responsible ways
Lack of remorse
Overinflated sense of self
Superficial charmLack ability to empathize
Prevalence
- Observed in 3.6% of the population
- More common in males
AUTISM SPECTRUM DISORDER
Symptoms
Deficits in social interaction (e.g., do not make eye contact, turn head away when spoken to, prefer playing alone)
Deficits in communication (e.g., one word responses, difficulty maintaining conversation, echoed speech, and problems using and understanding nonverbal cues)
Repetitive patterns of behavior or interests
Prevalence
Affects approximately 1 in 88 children in the U.S.
5 times more common in boys
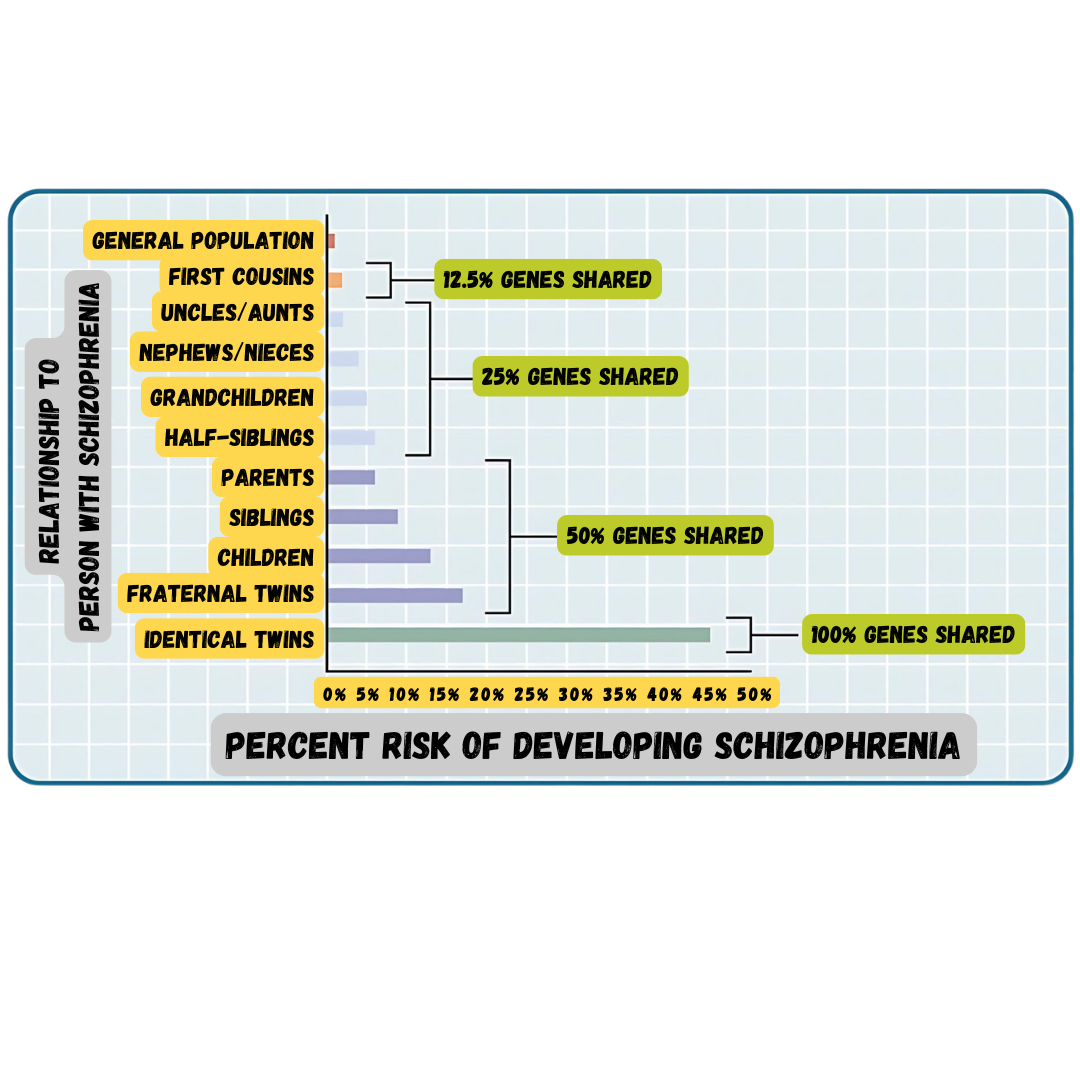
Genetics:
Identical twins – 60%-90% concordance rates
Fraternal twins – 5%-10% concordance rates
Genes involved are those important in the formation of synaptic circuits that facilitate communication between different areas of the brain
Environment:
- Factors that contribute to new mutations (e.g. pollutants)
![]()
SOCIAL ANXIETY DISORDER
Prevalence
Comorbidity
Risk factors
Fears of social situations possibly developed through conditioning
Most report history of severe teasing in childhood